
Living with Sjögren's syndrome: Sue's story

In 2012, Sue had a fall in the shower and struck her neck and back. She was ‘black and blue’ and feared she had a fracture. When she arrived in the Emergency Department in Gloucester, despite experiencing pains in both her chest and back, only her chest was X-rayed.
Two months after the fall, Sue was still experiencing a great deal of pain without receiving a diagnosis or explanation from health professionals. She saw a private doctor who suggested she have a spinal MRI. She was taken to Cheltenham General Hospital later the same evening and put on a ward.
Sue had the MRI, but although the neurologist arrived to admit her, he did not come back until the day she was then discharged, saying there was no need to see her again. The following day, Sue was very unwell and her GP tried to send her back in to hospital.
After a six-hour wait in the Emergency Department, she was again discharged. Sue was informed at the time that the results of the MRI was normal. However, two months later (four months after the fall), the same MRI image was reviewed by a Rheumatologist at Cheltenham General who identified a possible fracture on Sue’s T4 vertebra.
A subsequent X-ray confirmed a healing fracture. Sue said that the only time that this fracture could have occurred would have been at the time of her fall.
Over the next two years, Sue experienced 'terrible' nerve-related symptoms which she reported to health professionals. She feels that in some instances, the seriousness of this had been downplayed.
Patronising [...] abrupt manner [...] we are not all imagining it or making it up.
At the time and since her fall, all that had been briefly discussed was the possible fracture in her back. Sue said that the reasons behind the neurological symptoms had not been treated objectively or given enough consideration.
The nerve pain had a significant impact on Sue, affecting her quality of life and led to her having to give up her job and income. Her work required her to be fit and active, which she had been prior to the injury. Sue also considers herself to be a well-adjusted individual, who was not seeking unnecessary attention.
Throughout her experiences, Sue reported a great deal of trouble and frustration convincing neurologists that she was not delusional, and that her situation needed to be treated as something relating to physical/ neurological damage rather than psychological.
Since all this began, she has had a daily struggle with simple things, such as:
- swallowing
- experiencing sneezing which triggers sensations of cold
- constant twitching, tingling, cold patches on her legs and feet
- crawling sensations in her head
- temperature problems.
These symptoms have caused several trips to the Emergency Department and home visits from out-of-hours paramedics. For example, a flare up of swallowing difficulties can result in suffering a choking episode. However, Sue found that her concerns were dismissed as anxiety and 'being in her mind'.
Sue insisted on being referred to the National Hospital for Neurology and Neuroscience (NHNN) in London because health services in Gloucestershire seemed unable to find the cause of her condition.
15 months after her fall, Sue went to London for an appointment with a senior registrar at the NHNN. They had already read her notes from the NHS in Gloucestershire, and she felt that her lived experience of her symptoms and the impact they were having on her daily life were not given due consideration. She was referred to a pain management clinic rather than having the root causes of her symptoms investigated.
Sue felt that no-one was taking her seriously. Rather than having a mental health condition, Sue felt that it was these ‘patronising’ attitudes and ‘abrupt manner’ from health professionals that were causing her mental and emotional health to deteriorate. She wrote to the NHS in Gloucestershire in 2014 to ask for answers, but did not feel that these were forthcoming.
Sue had been seen by eight specialists across Cheltenham and Gloucester, including Gastroenterology and ENT, who identified that Sue had no saliva, but did not make a referral to investigate this further. After seeing a Skin Specialist who diagnosed her with a Lupus rash, Sue noted that they had written "Sjögren’s". Yet once again, no referral was made.
Sue reached out to Sjögren’s UK, and on their advice, she saw a consultant in Swindon and got diagnosed privately in 2014, 2 years after the fall which triggered symptoms. The consultant is one of five experts in Sjögren’s syndrome in the country.
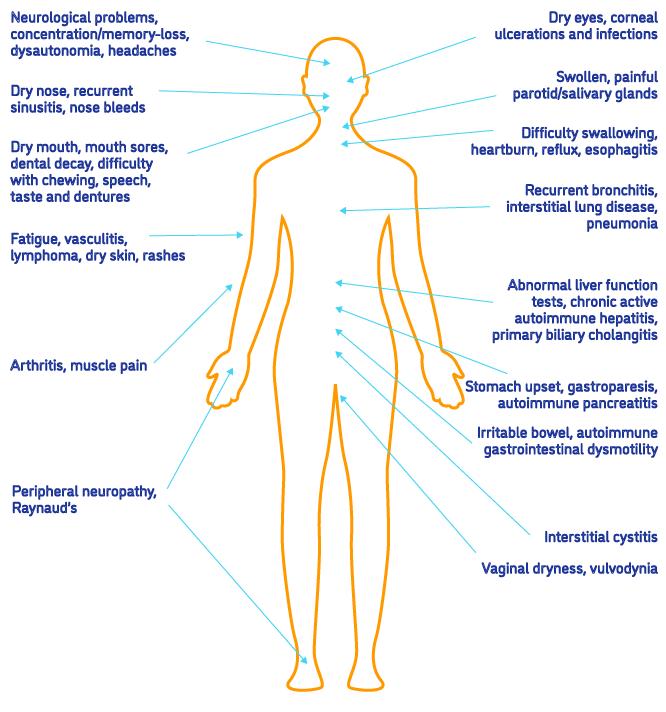
What is Sjögren's syndrome?
Sjögren's syndrome (also known as Sjögren's disease) is a condition where the glands that produce fluid, such as tears and spit (saliva), stop working properly. It can affect daily life, but treatments can help ease the symptoms.
There are lots of possible symptoms of Sjögren's syndrome and the condition affects people differently. It affects approximately 0.6% of adults in the UK, with an average age of 50 years. 90% of people diagnosed with Sjögren’s syndrome are women.
There's currently no cure for Sjögren's syndrome, but there are treatments that can help manage the symptoms. The type of treatment will depend on the symptoms someone has and how they affect them.
Sue’s diagnosis followed a negative blood test and a positive lip biopsy result. A negative blood test can occur in many Sjögren’s patients resulting in them being discharged from services.
Since having her diagnosis, Sue continues to experience dismissive attitudes and fears needing to receive urgent and emergency care and being under the care of doctors in Gloucestershire who have no awareness of the condition and therefore misdiagnose her symptoms.
She is currently under five different consultants at Great Western Hospital in Swindon to manage the many symptoms she experiences as a result of Sjögren’s. This relies on her being able to drive and afford the fuel and parking, as well as taking time out of her life and caring responsibilities.
Sue is fully aware that not everyone is in this position and in fact she supports some group members to be able to attend their appointments by driving them to Swindon and back. Sue has also struggled to access the medication that treats her symptoms most effectively in Gloucestershire.
She has been offered different brands of the same medication, but as they manufactured differently, different brands can cause her symptoms to flare up and make her feel worse. She is able to get the medication that works for her from Swindon, so has the expense of needing to travel there to get her prescriptions.
Experienced medics tried to dismiss every single problem she was having and Sue holds them responsible for causing further nerve related damage.
She has autonomic problems associated with Sjögren’s, and should have been placed immediately on the six-month waiting list from the onset. She feels that there were many markers indicating that there was a serious health problem going on - but no one seems willing to look at all these symptoms in a holistic way.
Sue strongly believes it would be beneficial if health professionals listened properly to patients and believed in what they were saying - especially older patients as "we are not all imagining it or making it up."


